

Lauren Beasley – contributing writer for Breaking Muscle!
The butt-wink, the slouch, and the rounded back. Snooze. We’ve heard time and time again that these positions are bad. Hopefully, if you haven’t already corrected these dangerous, faulty, and weak (did I say dangerous?) patterns, you are making significant strides.
During a squat, you might be trying to work on keeping your chest up, sending your butt back, and keeping an arch in your lumbar spine, as these movements are typically lacking in a rounded back dysfunction.

Coincidentally, those same three frequently used cues are fairly accurate in describing the unsteady, overextended waddle of a toddler taking his first steps. While I don’t want you to flex your spine into a herniated disc, round your shoulders forward into anterior instability, or shorten your hamstrings by tucking your pelvis under, I most certainly don’t want you walking around like some novice ambulator. The toddler stance may save you from the potential repercussions of flexed positions, but this alternative is no lesser of two evils. An overextended posture and movement dysfunction sets you up for equally disastrous injury risk.
The Dangers of the Toddler Stance
The Toddler Stance – or overextended posture – describes an anterior pelvic tilt, an extension of the thoracolumbar (lower thoracic and lumbar) spine, and usually some hyperextension of the knees. While not ideal for adults, this posture is useful to toddlers as they learn to walk because their body has yet to develop the strength necessary to support good, efficient walking.
Instead, toddlers seek stability by locking out and hanging on ligaments and joint capsules of the knees and lumbopelvic complex. They rapidly grow out of this stage as they develop better strength and balance – right around the same time they start to execute the perfect squat we all strive to recreate. Adults, however, have a much harder time kicking the overextension habit, relying on this strategy to compensate for much more than an unsteady gait.
An Attempt to Fix Core Instability
Overextension is our solution to core instability. Through hanging on structures of the lumbopelvic complex, an athlete can create a stabile midline and go on to achieve whatever greatness he or she is destined for. Specifically, the prong-like facet joints that interface between two adjacent vertebrae lock in when you hold yourself in extension. But we all know that structures only do what your muscles allow them to do, and in this situation that means the spinal extensors along with their buddies the hip flexors are doing a lot.
The toddler stance often appears on heavy back squat day. Watch someone step under the bar, rack the weight, and descend. Those who are not rounding are likely overextending. Using those hip flexors and lumbar extensors, the overextender shoots his hips back until his previously hyperextended knees can hinge into flexion, as the spine forms the exact shape of a knock-hockey stick. Overextension gets the job done and as an added bonus is way less likely to get you called out by your coach, but like all movement dysfunctions, using your body incorrectly means that you are inherently missing out on optimal performance. Of even greater importance, incorrect stabilization strategies predispose you to injury risk.

In overextension, the amount of compression loaded onto the lumbar facet joints skyrockets, which over time with repetitive loading can lead to a stress fracture of the spine called spondylolysis. Spondylolisthes, a similar condition, involves actual displacement of a vertebra, usually after both facet joints of the same level fracture as a result of the undue strain. This sounds bad, but only because it is bad. More commonly, overextenders are likely to get that “pinchy” feeling in the front of their hips, or impingement. Just as with shoulder impingement, faulty mechanics of the hip joint creates a physical compression – in this case usually the rectus femoris, part of your quads. Additionally, with your center of gravity displaced forward by overextension, the lower extremities are forced to make adjustments to keep you upright. Pick your poison – they are all potential products of the toddler stance.
When Toddlers Go Overhead
Overextension clearly creates local mayhem at the lumbopelvic complex and can initiate chaos in the lower extremities from a top-down domino effect, but your upper half is not out of the woods when you look at what happens from the bottom up. In fact, some of the worst overextenders maintain good control over their lower half and instead, these individuals rely on the toddler stance to compensate for another dysfunction.
Athletes who have difficulty with overhead movements commonly recruit an overextended position as a secondary dysfunctional pattern. Restrictions of upper thoracic extension, loss of shoulder flexion, and scapular instability are all potential contributing factors limiting overhead capacity, inviting an overextended posture in to pick up the slack for both mobility and stability deficits.
For athletes lacking range of motion as well as control, the toddler stance allows the athlete to “balance” weights overhead – keeping the weight directly in line with the base of support (the feet). As an added bonus for athletes lacking overhead mobility, overextension creates a false range of motion at the shoulder that is useful when trying to hold, push, or catch heavy weights overhead. The problem with balancing weights overhead is that you are doing just that – balancing – instead of owning that weight and maintaining control.
Sloucher by Day, Badass by Night
Lastly, and most ironically, many overextenders are also slouchers. Yes, these special folks use two contradictory strategies to achieve one common goal – stability. By day, these guys are probably your average desk-jockeys, slumped over a computer, hanging on their overstretched spine. By night, they transform into badass metal-moving mo-fos, overextending and locking out their spine to press an excessive weight overhead. This is a recipe for disaster. Compressing structures and using muscles incorrectly is exactly how you wear and tear your way to surgical repair.

Slouching – the most recognizable of the bad postures – is certainly not the only bad position, and definitely not the only dysfunction that comes with risks. For some of you, the toddler stance dilemma is like that of the chicken and the egg. Was your shoulder dysfunction the gateway drug into overextension? Or did your overextension lead you to believe that your arms were fully overhead when really they had ten degrees to go? For those of you battling the “butt wink” and avoiding a rounded back like the plague, perhaps a misunderstanding of where the middle is led you to inadvertently create a new dysfunction.
Regardless of how you found yourself in overextension, do yourself a favor. Find neutral. Unload your spine. Decompress your hip flexors. One thing is for sure – the only people who should be walking around in overextension are nine-month pregnant women, curve-embellishing tweens, and actual toddlers.

Lauren Beasley – contributing writer for Breaking Muscle!
We all have our weaknesses. You know, those things you skip out on or (not-so) silently protest when you see them programmed into your workout. Come early and stay late to tackle your goat? Maybe tomorrow. Only you can make excuses for why you haven’t nailed the double under or conquered a strict pull up. But I can give you some reasons as to why – despite your best efforts – you are not getting stronger.
Body Awareness
For those of you who leave the mind-body connection to the Zen masters of the world, now is your chance to understand why you, too, need to be one with your body. Body awareness, or proprioception, is your body’s position sense and the key to successful movement. Close your eyes. Is your left knee bent or straight? How do you know? You just know, right? No. Proprioception is how.

Someone once asked me, how could a person be “good” if they don’t know what “good” looks like? At the time, this advice was intended to motivate me to lead my staff by example, but I later realized this person was 100% right. I’m sure this was great general boss-employee advice, but I’ve found that this is also some of the best advice for movement. If you don’t know what good looks like – or better yet feels like – you don’t have a working model to help guide your behavior.
“Pinch your shoulders back,” “Pull your ribs down,” and, “Reach your tailbone back,” are a few examples of cues that are usually met with blank stares. Pinching shoulder blades often turns into a shrug, pulling ribs down looks like a crunch taking the shoulders along for the ride, and people trying to reach their tailbones back look like they are auditioning for Soul Train. Even some of my best athletes have no idea what “good” looks like and they certainly have no clue as to what “good” feels like. So, if you don’t know what to feel, how can you activate and strengthen those muscles? This is reason number one you aren’t getting stronger.
Movement Patterns
You might be starting to pick up on the fact that I’m a huge physical therapy nerd, but long before I was geeking out about anatomy and movement, I was a different kind of nerd. I was in the band. In the seventh grade, I was selected to play the clarinet in an all-county orchestra comprised of other nerds, just like me. All of us talented (awkward) individuals were given sheet music ahead of time so we could learn the song. When we assembled as a group, we divided into sections (winds, horns, strings, etc.) and began to practice. Gradually, we started to integrate all of the parts into a whole, but not without help.
The most important member of the orchestra was not a single musician, but instead was the conductor. With his baton, he signaled how fast or slow to play, when to get louder or softer, and when to cue in a solo performance. Eventually we memorized our parts and relied less on the conductor’s guidance, but at any given moment with one wave of his baton he could make us speed up and get loud, or slow down and get soft. He was the regulator. Without him, the horns section might have played at the wrong time, or a violinist might have forgotten her solo. The conductor coordinated our individual strengths into a strong, successful performance.

Here’s what I’m getting at: every time we move, the body performs an intricate masterpiece. Individual muscles team up to create a kinetic chain, and then these groups of muscles work with other groups of muscles to do something as simple as turning off a light switch. Seems complicated, but lucky for us, just like the orchestra we have a guy standing up front waving his baton. That’s the cerebellum. The cerebellum is in constant communication with muscles like a circuit, moderating movements using proprioception. When we learn new movements, the cerebellum gets involved – a lot. As movement patterns become more established, our muscles rely less on higher-level intervention and more on memory. Muscle memory. Good patterns or bad patterns, these will be the strategies you body remembers – and uses.
During your waking hours, you have two choices: reinforce good habits or reinforce bad habits. What you do fifteen hours a day always trumps what you do fifteen minutes a day, so pay attention to what you do outside of training just as much as what you do during a session. It is never too late to teach your muscles how to work together to produce better, more efficient movement patterns. Using poor habits is the second reason you aren’t getting stronger – you are using the wrong muscles at the wrong times to execute a movement. Otherwise known as cheating.
Inhibition
If I told you to pick any three movements to perform, odds are pretty good you would choose three movements you are good at. Maybe a few overachievers would throw a weakness into the mix because “you know you need to work on it.” But let’s assume you are like the rest of us. You give me your three best movements because those are your strengths and the actions you feel most confident performing. This is human nature. Tiger Woods didn’t turn down the NBA to work on his golf game. He played to his strengths. We all do it. Your body does it, too.
Pinching shoulder back turns into a shrug. This example can be explained by poor body awareness (reason number one), incorrect movement patterns (reason number two) or our third reason, inhibited muscles. You’ve got upper traps that could shrug a refrigerator, but your middle traps are mediocre at best. When I ask you to pinch your shoulder blades back, how could you not shrug?
Just like you gravitate toward your strengths, your body defaults to the muscles and movement patterns it feels most confident with. With upper traps dominating this movement pattern, no matter how hard you try you can’t pinch your shoulders back without shrugging. In this scenario, your upper traps are overriding, or inhibiting, your middle traps and often times these compensations are not obvious. When you use the wrong muscles to get a job done – even unintentionally – you are not going to achieve your full potential.

Take Home
Over the course of your life, you’ve learned how to move in an astonishing number of ways. Not all of the ways you move are correct, in fact some of your habits are probably downright horrific. But that doesn’t stop you from moving. When you ask your body to do a job, your body doesn’t care what it looks like – it carries out an order using the resources it has available and the habits you have developed over the years. If you have poor body awareness, poor movement patterns, and the wrong muscles are inhibiting the right ones during your performance, if you haven’t already hit a plateau in strength, then there’s a good chance one is coming your way. And usually, injury is not too far behind.

I cannot thank you enough for your commitment to my recovery from hip surgery and getting me back to one hundred percent. I feel your personal approach to treating patients is unmatched anywhere and has ultimately allowed me to progress quicker than I could have imagined – one month ahead of schedule! After 5 months of PT my hip is feeling the best it’s felt in two years and I am finally back to doing all the things I love to do in the gym: squatting, deadlifting, running and jumping- all pain free!

Lauren Beasley – contributing writer for Breaking Muscle!


Strength and stability are different. I address strength with mobility for the simple reason that a muscle needs to be strong enough to produce movement. Having enough strength to move is not the problem for most people. Stability on the other hand is more advanced and although the act of stability is difficult, the concept of is simple – hold still. We achieve stability through co-contractions. What happens if you squeeze your push muscles at the same time that you squeeze your pull muscles? Muscles are pulling equally on opposite sides of a joint, like a dead heat of tug-of-war. Nobody moves. You’ve got stability!
 When you combine stability and mobility, you get controlled mobility. Hold something still and move something else. Stabilize your core, and raise your arm. Controlled mobility yields functional movements that we use throughout our life and demands a dynamic stability, changing in response to the movement. Dynamic stability is more like a well-matched game of tug-of-war. Teams on either side of the rope take turns dominating the game, moving the red flag in the middle, but never let tension of the rope release.
When you combine stability and mobility, you get controlled mobility. Hold something still and move something else. Stabilize your core, and raise your arm. Controlled mobility yields functional movements that we use throughout our life and demands a dynamic stability, changing in response to the movement. Dynamic stability is more like a well-matched game of tug-of-war. Teams on either side of the rope take turns dominating the game, moving the red flag in the middle, but never let tension of the rope release.
[youtube]http://www.youtube.com/watch?v=-y3PBdjQLho[/youtube]
[youtube]http://www.youtube.com/watch?v=DGr3pq07Jrc[/youtube]
Lauren Beasley – contributing writer for Breaking Muscle!
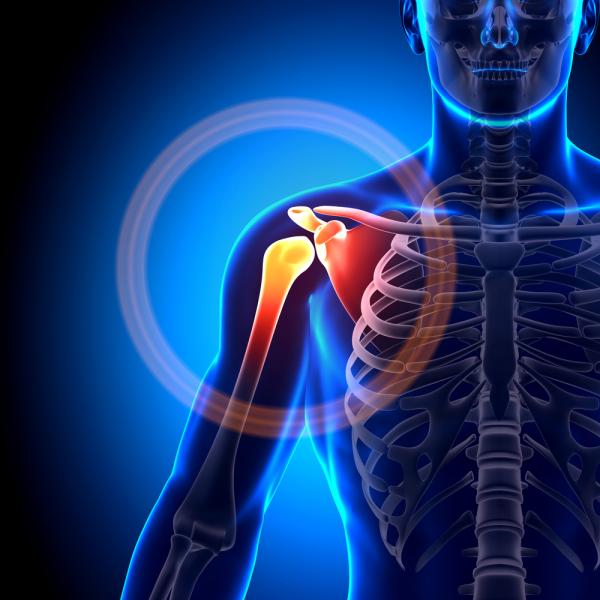
Some things just go together. Peanut butter and jelly. Jordan and Pippen. Cheech and Chong. You could have one without the other, but things just wouldn’t be the same. In the body, arguably the biggest power couple is the ball and socket – a term synonymous with the shoulder. But in the body we don’t just have great duos, we have amazing kinetic chains. PB&J would never have made it big without the bread (pre-paleo). Phil Jackson was the one who merged two megastar individual talents into the synergistic backbone of the Chicago Bull legacy. And Cheech and Chong? Well, we all know what their magic ingredient was.
My Shoulder Has a Complex
While the term “shoulder” most commonly refers to the ball and socket mechanism, the shoulder complex actually consists of multiple joints:
 The first, and only “hard” connection between our arms and axial skeleton (skull, spine, ribcage, and sternum) is the costoclavicular joint, or where the collarbone meets the sternum.
The first, and only “hard” connection between our arms and axial skeleton (skull, spine, ribcage, and sternum) is the costoclavicular joint, or where the collarbone meets the sternum.- Following the clavicle away from midline – distally – the next union is our acromioclavicular joint (AC). Here the clavicle sits on top of a projection from the scapula called the acromion process. When the shoulder is “separated,” this is where that dislocation occurs.
- No introduction is necessary for the next joint in line, the ball and socket, or glenohumeral joint (GHJ).
- Although not technically a real joint, the final articulation in the shoulder complex is the scapulothoracic joint (STJ), or the “connection” between the shoulder blade and the thoracic spine and associated ribs.
Together, this intricate cluster of joints creates the incredible shoulder – the cornerstone of movement through the upper extremity. But like any great team, many do the work while few get the credit. Ask Jordan or Pippen.
The Roles of the Joints in the Shoulder Complex
 The glenohumeral joint is the MVP of our shoulder complex. It’s flashy, makes the big plays, and scores all the points. The GHJ joint is the single most mobile joint in the body. But, thanks to the laws of physics, mobility exists at the expense of stability. Picture a golf tee and a golf ball – this is the age-old analogy that best describes the dimensions of the GHJ joint. When the tee is set just right, the ball can sit perfectly centered in the shallow support of the tee. As long as the ball doesn’t keep falling off the tee, you can now step up to the box and drive the ball in just about any direction you want, with the exception of straight down. Works great for golf, but how can such an unstable joint work in our body? Simple. The glenohumeral joint can only be so amazing with the help of the scapulothoracic joint.
The glenohumeral joint is the MVP of our shoulder complex. It’s flashy, makes the big plays, and scores all the points. The GHJ joint is the single most mobile joint in the body. But, thanks to the laws of physics, mobility exists at the expense of stability. Picture a golf tee and a golf ball – this is the age-old analogy that best describes the dimensions of the GHJ joint. When the tee is set just right, the ball can sit perfectly centered in the shallow support of the tee. As long as the ball doesn’t keep falling off the tee, you can now step up to the box and drive the ball in just about any direction you want, with the exception of straight down. Works great for golf, but how can such an unstable joint work in our body? Simple. The glenohumeral joint can only be so amazing with the help of the scapulothoracic joint.
The scapulothoracic joint is the bread to our PB&J, our Phil Jackson to Jordan and Pippen, and the fuel to Cheech and Chong’s fire (or should I say smoke?). Without the scapulothoracic joint, the glenohumeral joint would be rendered useless. The relationship between these two joints is all too often overlooked when addressing the shoulder as focus is instead shifted to the ball and socket (alone) or the scapula (alone). The coupling of the GHJ and STJ effectively links the arm to the thoracic vertebrae meaning dysfunction of the spine can compromise the shoulder – and vice versa.
The Scapula and Stability
 Here’s how the dots connect. Starting from midline, the thoracic spine forms a column from which twelve ribs attach. These ribs wrap around in a barrel-like fashion, creating the rib cage. Consider the thoracic vertebrae the foundation under a building and the ribs the floors sitting on top. The triangular-shaped scapula sits on top of the ribs, just as a rug would lay flat on a floor.
Here’s how the dots connect. Starting from midline, the thoracic spine forms a column from which twelve ribs attach. These ribs wrap around in a barrel-like fashion, creating the rib cage. Consider the thoracic vertebrae the foundation under a building and the ribs the floors sitting on top. The triangular-shaped scapula sits on top of the ribs, just as a rug would lay flat on a floor.
At rest, the superior border of the scapula runs horizontally from shoulder to spine and then turns down at a ninety-degree angle continuing parallel to the spine as the medial border of the scapula. A little more than midway down the spine the scapula turns up, becoming the lateral border as it heads up and out toward the armpit where it meets the superior border to complete the triangle. This junction of the superior and lateral border creates a projection called the glenoid fossa, which you know as the socket. The glenoid holds the ball, which is the rounded end of the humerus bone, to form the glenohumeral joint.
Say we are moving furniture into a building. We require that a solid foundation provide the base for our building. Then, flooring would need to be installed so that we can lay down a rug. Only after these steps are taken – in this order – furnishings can be brought in. Similarly, we must ensure a stable spine and ribcage for the scapula to sit on so that it can in turn be a reliable support for the arm. Stability at each and every link along this kinetic chain is necessary for function as a whole. Without Jordan bringing his A-game, Pippen performing to full potential, and Phil Jackson calling all the right plays there is no three-peat championship for the Chicago Bulls.
The Muscles Involved With the Shoulder Complex
 The good news is that we are much more like the Bulls than a building. While we ideally have “good bones” like a building, that’s where the similarities end. We are more than a skeleton. We don’t sit idly. We don’t break and not bend. We are dynamic. We act and react. We can take our sturdy foundations and move them in all kinds of ways, producing amazing feats – like drilling the game winning three-pointer at the buzzer. But, as important as our bones are, we can only control what they do with our muscles. When it comes to operating the shoulder complex, the rotator cuff, scapular stabilizers, and core muscles are in charge. Without these muscles, we are just an idle structure.
The good news is that we are much more like the Bulls than a building. While we ideally have “good bones” like a building, that’s where the similarities end. We are more than a skeleton. We don’t sit idly. We don’t break and not bend. We are dynamic. We act and react. We can take our sturdy foundations and move them in all kinds of ways, producing amazing feats – like drilling the game winning three-pointer at the buzzer. But, as important as our bones are, we can only control what they do with our muscles. When it comes to operating the shoulder complex, the rotator cuff, scapular stabilizers, and core muscles are in charge. Without these muscles, we are just an idle structure.
Stability of the glenohumeral and scapulothoracic joints occurs in a specific order. First, the thoracic spine moves (or doesn’t) thanks to our core muscles. Then, our scapula is anchored to the spine and ribcage via several different stabilizing muscles. Lastly, the rotator cuff travels from the surface of the scapula, crossing the glenohumeral joint to hold the ball into the socket. Centered around the scapula, these three groups of muscles work together as a kinetic chain connecting the core to our upper extremity. The scapulothoracic joint, as a result, is the key to the shoulder. Insufficient stability of the STJ is the main ingredient in the recipe for disaster – and not just at the shoulder. Inability to control the scapula can lead to neck pain and headaches. Weakness of the shoulder blade not only decreases the ability for the arm to function, but it can also bring us down, literally. A slouched posture and overextended spine can both result from weakness at the scapulothoracic joint.
Control your scapulothoracic joint, and you control your ability to make gains with strength and power, abolish or avoid pain and dysfunction, and most importantly, take a huge stride toward mastering the complexity of human performance. Controlling your STJ is easy, and I’ll show you how. Next time.

Total Physical Therapy & Lauren Beasley changed my life. I am enormously grateful. I came to TPT after “resting” a chronic hip injury for 14 months based on my doctor’s advice. The injury stagnated and would not resolve itself. From the initial phone consultation, Lauren Beasley of Total-PT was engaged, enthusiastic, and confident she could improve the situation and get me back to running and normal fitness activity. Having now successfully completed my physical therapy program, I am now back to my pre-injury activities and completely thrilled with the entire experience. There is no substitute for the personal, one-to-one approach Total-PT takes to it’s patients. The therapist is not circulating from one patient to another during your session. You are the sole focus for that hour. The exercises and techniques are tailored to you, how you are feeling that day/week, and what the right next progression is. Lauren Beasley was excellent at explaining the reasons for the therapy she recommended, how it relates to anatomy and biomechanics. She was also available and happy to chat or text between sessions if something came up. It is true personal service, and done with a great attitude. I would recommend Total Physical Therapy to anyone who is committed to resolving an injury through exercise and improving their strength, mobility and flexibility.

Thanks Lauren! Christian just called. He set a personal record tonight in the 400 meter at the NYC armory. He ran a 50.6 and got a silver medal. He was the only Seton Hall Prep runner to qualify for the Eastern States later this month. All this with no practice in the last three weeks! He thanked God first, and you second!
Much appreciated!


Here’s Lauren Beasley’s follow-up article as featured in Breaking Muscle
We need stability in much the same way that we need air. We need to supply oxygen in the right amounts, at the right times, and according to the demand. It’s a simple supply-demand relationship and the same goes for stability. For years, the core muscles (read: abs) have been the focus of stability training and with good reason. The muscles traditionally referred to as “the core” provide a working surface for our extremities to push off of, which is crucial for any kind of movement, from throwing the game-winning touchdown pass to signing an autograph after the victory. You’d be hard pressed to find someone with a good argument for not training core stability.
 But there’s more to the story. The core is where we generate, absorb, and transfer forces to and from our extremities, which means we need to focus on stabilizing the connection between extremity and core. Enter the hip.
But there’s more to the story. The core is where we generate, absorb, and transfer forces to and from our extremities, which means we need to focus on stabilizing the connection between extremity and core. Enter the hip.
In my last article, I shared knowledge that came from years of seminars, textbooks, mentorships, and trouble-shooting all kinds of injuries. I revealed that hip instability is the common thread of so many problems – from back pain to shin splints – and sub-par hip performance is far more common than you might think. But unless you’re in a serious state of denial, admitting that your hip isn’t working so well is not the hard part – fixing it is. So, let’s make this simple. I’m going to break fixing your hips down into five steps:
Step #1: Deep Tissue Mobility
I know, you expected strength and stability drills, but before you ask your muscles to work, you should probably make sure they are able to work. Foam rolling and lacrosse ball mobility drills have become all the rage, but while “everyone’s doing it” is a good enough reason to get most people on the bandwagon, understanding the purpose and value of these drills will help prioritize when and where you should spend time suffering through deep tissue mobility work.
When a muscle is tight, range of motion can be compromised. Lack of range of motion causes changes in movement patterns that limit quality of performance and ultimately create injury risk. A tight muscle is a weak muscle. An overstretched or long muscle is also a weak muscle. This conundrum is known as the length-tension relationship. In short, this rule says that a muscle must be at mid-length (or on a slight stretch, to be exact) to generate optimal force. If a muscle contracts by shortening, how can the muscle generate force if it is already shortened? This concept applies not only to overall length of muscles, but to isolated units within a muscle.

We know that several muscles play an intricate role in supporting the hip joint, but I’m going to play favorites and pick on the gluteus medius. Not just because it is notoriously tight, but because this is the most common source of breakdown I come across in the clinic. And the glut med is no job for a foam roller – too close for missiles, Mav, better switch to guns. Due to its smaller surface area, the lacrosse ball is the perfect tool to dig into the lateral hip and provide enough pressure to release the fibers. Spend a few minutes on each side, and consider your glutes ready for action.
Step #2: Isolated Strengthening
Turns out, there is a purpose for those wimpy isolation exercises that have been shunned by the fitness world in lieu of functional training. (Don’t worry – we’ll get to that, too.) After step one, you’ve smashed, mashed, and rolled your hip fibers into prime shape for work, and while they can now create a stronger contraction, they are clearly still weak. This second step is not a quick fix and requires some good old-fashioned hard work. Cue: targeted, remedial strengthening.
Before I step into the lion’s den by singling out some exercises, let’s get a few things straight. First, I have read many studies examining the best way to elicit hip muscle activity and there are a lot of conflicting results. Regardless of the exercise, a major factor in the effectiveness of targeting a specific muscle is cuing and awareness. In other words, if a person tries to squeeze their glutes during an activity, then the glutes are more active. Second, if a person has weak glutes, then pretty much any method of targeting glute strength will do, as anything is better than nothing. Lastly, anything is better than nothing also applies to compliance. If an athlete isn’t going to do the exercise then it’s not very effective, is it? So let’s keep it simple and easy to perform.
While this overview of hip strengthening methods is far from comprehensive, no list of lateral hip exercises would be complete without side-lying abduction. After all, this is the primary “action” of the glute med when the muscle fibers concentrically contract. Additionally, side planking is an excellent way to isometrically fire the glute med as the lateral hip muscles keep you off of the ground. Want to get fancy? Hold a side plank and perform abduction with the non-weight bearing leg.
Step #3: Functional Strengthening
 Moving right along! Your glute med is now willing and able to work, so the important focus now becomes retraining this muscle to work functionally. In weight bearing, the glute med must fire to stabilize the pelvis, mainly in unilateral stance. Therefore, I recommend targeting the glute med in weight bearing with focus on double- and single-limb stance.
Moving right along! Your glute med is now willing and able to work, so the important focus now becomes retraining this muscle to work functionally. In weight bearing, the glute med must fire to stabilize the pelvis, mainly in unilateral stance. Therefore, I recommend targeting the glute med in weight bearing with focus on double- and single-limb stance.
A simple way to ensure the glute med is firing as you weight bear is to use a resistance band around the ankles or knees while walking. Forward, backwards, laterally – whatever method suits your mood. Lateral step-ups and single-leg Romanian deadlifts also work well to functionally train the glute med.
Step #4: Dynamic Stabilizing
Continuing along this progression, it is now time to make sure we can supply hip stability in the right amount, at the right times (just like oxygen). Plyometric work such as speed skaters and single leg work in the form of broad jumps or box jumps require the glute med to stabilize the pelvis during more dynamic activity. This is challenging, but struggling with this stage is necessary in order to carry over good movement patterns established in simple, controlled activities to more unpredictable situations.
Step #5: Skill
Here’s the fun part. How you choose to use and challenge your shiny new hip stability is up to you. Your sport will guide the next steps in training your hip to ensure your stability is up to par for the specific demands you place on your body. Remember, breaking down complex skills into their smaller parts is crucial to successful performance. Perfect practice makes perfect.
That’s it. A systematic approach to tackle movement dysfunction. Using this logic, now you can apply your own tried and true techniques. (Spoiler alert: this also works pretty well for our other core-extremity connector, the shoulder.)
Total Physical Therapy is proud to announce our inclusion as a featured practice on Back to the Box. Back to The Box is a membership-based website that serves highly motivated functional fitness, competitive and tactical athletes recovering from orthopedic surgery or injury. BTTB provides online rehabilitative training programs and recovery education to include written and video content. Back to the Box is based out of Durango, Colorodo and has over 400 facilities nationwide that provide elite services to athletes and the military elite. We are the only providers in the state of New Jersey. You can find out more by going here.

Congratulations to our own Lauren Beasley! She has become a contributing writer for the popular online publication Breaking Muscle! Here’s her 1st article:
I’m on to you. You’re not here to read. You’re here to improve. You want to train better, perform better, feel better – whatever your better may be. You are willing to suffer through this article hoping to add just a little bit more knowledge to help you achieve your better. You are also smart enough to know there are no quick fixes or shortcuts, so you’re willing to work. Hard. But in spite of your impressive dedication and awe-inspiring work ethic, you still want better as fast as possible.
Since I know your secret, I’m going to let you in on one of mine. I want to tell you the one thing I see over and over again. The one difference between good performance and maximizing performance potential. The one thing that can be the difference between staying healthy and getting injured. And because you are so smart, you ask, “Why should I listen to you?”
 Here’s what you need to know: I am a physical therapist who works almost exclusively with athletes. From lacrosse players to CrossFit, from recreational to the very elite, these are the individuals with whom I work day in and day out. I left the humdrum world of ultrasounds, icepacks, and ankle-cuff weights to work with the most motivated clients and best teachers – athletes. All day every day I work one-on-one with athletes watching them move and problem solve their way (back) to 100%. And over and over again I see a common thread limiting my athletes, their Achilles heel – the hip.
Here’s what you need to know: I am a physical therapist who works almost exclusively with athletes. From lacrosse players to CrossFit, from recreational to the very elite, these are the individuals with whom I work day in and day out. I left the humdrum world of ultrasounds, icepacks, and ankle-cuff weights to work with the most motivated clients and best teachers – athletes. All day every day I work one-on-one with athletes watching them move and problem solve their way (back) to 100%. And over and over again I see a common thread limiting my athletes, their Achilles heel – the hip.
Almost all of the cases I treat stem from lack of core stability – specifically, from the lateral hip musculature (and yes, I group hip muscles into the core). Certainly you could see how this may be true if I were to only specialize in lower extremity treatment, but since I am telling you one of the secrets to my success, you should know that hip dysfunction also explains almost all of my waist-up cases (the technical term). As we go about our day-to-day lives moving from point A to point B, much of our activity requires us to move forward, or in the sagittal plane. Marathon runners, swimmers, point guards, and quarterbacks all have their eyes on the prize, in front of them. In order to produce any movement in this front-to-back plane, we must be able to use our lateral stabilizers, or anti-rotators, in the right amount, at the right time. Piece of cake, right? Now stabilize your core and control functional, diagonal, movements. Bob and weave, pivot and cut, juke your guy out of his cleats. Better have hips that would make Shakira drool.
The hip muscles – the glutes, the deep rotators, and yes those adductors that seem like they only exist to cause problems – are collectively charged with the daunting task of stabilizing everything above and below the hip. For example, as we walk, when we stride forward the standing hip must provide the force needed to prevent our torsos from dropping side to side and hold the hip and pelvis stationary (relatively speaking) to allow the knee to perform the simple hinge action for which it was designed. With such a large role, you can easily see how individuals of all abilities would have difficulty successfully controlling this multi-planar joint and the real trouble begins when compensations set in.
 Let’s start with the Trendelenburg gait. This is a dysfunctional movement pattern we physical therapists are taught ad nauseam and love to point out during gait analysis. “Ooh, ooh! His pelvis dropped to the contralateral side, Trendelenburg!” This gait pattern occurs due to weakness of primarily the gluteus medius. We learn that this hallmark sign of lateral hip weakness can be spotted when the non-weight bearing hip drops lower than the level of the standing hip. Since we go to school for a really long time, we also learn that some individuals will compensate for this weakness by leaning their torso toward the side of weakness. You can assess this by watching someone walk, or stand on one leg. In our advanced classes, we learn that the glute med (we are older and cooler, so we abbreviate now) is also a rotator and when it is weak, the knee caves into an ugly valgus position (pictured right) because the hip dropped into internal rotation, straining the medial aspect of the knee.
Let’s start with the Trendelenburg gait. This is a dysfunctional movement pattern we physical therapists are taught ad nauseam and love to point out during gait analysis. “Ooh, ooh! His pelvis dropped to the contralateral side, Trendelenburg!” This gait pattern occurs due to weakness of primarily the gluteus medius. We learn that this hallmark sign of lateral hip weakness can be spotted when the non-weight bearing hip drops lower than the level of the standing hip. Since we go to school for a really long time, we also learn that some individuals will compensate for this weakness by leaning their torso toward the side of weakness. You can assess this by watching someone walk, or stand on one leg. In our advanced classes, we learn that the glute med (we are older and cooler, so we abbreviate now) is also a rotator and when it is weak, the knee caves into an ugly valgus position (pictured right) because the hip dropped into internal rotation, straining the medial aspect of the knee.
When you zoom the microscope out, you can see that hip weakness looks like a lot of things, not just the Trendelenburg sign. Often, there are no deviations in sight and more importantly, the negative effects have far greater reach than just pain at the hip or the knee. My athletes have shown me time and time again that when one movement strategy fails, they have an arsenal of second and third-string muscles ready to take over. Being able to substitute muscles in a time of need makes for a great short term strategy, however if such compensations are sustained over time, you will eventually see a plateau in performance and breakdown of muscles that are doing someone else’s job in addition to their own. Have you ever had to pitch in a little extra to make up for a colleague or teammate? Sooner or later being taken advantage of will get old.
 Instead of demonstrating “down and in” collapse at the knee and ankle, the posterior tibialis at the inner shin can do a great job of lifting the arch and reducing the knee valgus. The posterior tib also excels in causing debilitating shin splints when used to do more work than it is supposed to.
Instead of demonstrating “down and in” collapse at the knee and ankle, the posterior tibialis at the inner shin can do a great job of lifting the arch and reducing the knee valgus. The posterior tib also excels in causing debilitating shin splints when used to do more work than it is supposed to. - The sartorius is an abductor and external rotator of the hip and with connections at the anterior hip and the medial knee, like the posterior tib, this long strappy muscle can pull the knee up and out when it contracts. Makes a good substitute for the glute med, right? Absolutely, with hip and knee pain to boot.
- If the glute max slacks off and lets your torso lean too far forward, the ankle plantarflexors are ready and willing and help hold you up. How much weight do you think your calf muscles can squat? You get the point.
The secret should be pretty clear by now – by mastering hip control in all planes, you can control whatever kind of movement you would like your body to create. You can be as static or dynamic as the hip allows. When the body works how it is designed, it is a powerful machine capable of both force and finesse. Big muscles do the heavy lifting while small muscles make minor adjustments. This results in efficient (read: strong and safe) movements. Control your hip, and you control your body.